 E-submission
E-submission
Search
- Page Path
- HOME > Search
Original Articles
- Additional nodules detected using EOB-MRI in patients with resectable single hepatocellular carcinoma: an implication for active treatment strategy
- Na Reum Kim, Seoung Yoon Rho, Jonathan Navarro, Chansik An, Dai Hoon Han, Jin Sub Choi, Myeong-Jin Kim, Gi Hong Choi
- J Liver Cancer. 2024;24(1):92-101. Published online February 14, 2024
- DOI: https://doi.org/10.17998/jlc.2024.01.25

- 903 Views
- 46 Downloads
-
 Abstract
Abstract
 PDF
PDF - Background/Aim
Gadolinium-ethoxybenzyl-diethylenetriamine pentaacetic acid-enhanced magnetic resonance imaging (EOBMRI) further enhances the identification of additional hepatic nodules compared with computed tomography (CT) alone; however, the optimal treatment for such additional nodules remains unclear. We investigated the long-term oncological effect of aggressive treatment strategies for additional lesions identified using EOB-MRI in patients with hepatocellular carcinoma (HCC).
Methods
Data from 522 patients diagnosed with solitary HCC using CT between January 2008 and December 2012 were retrospectively reviewed. Propensity score-matched (PSM) analysis was used to compare the oncologic outcomes between patients with solitary HCC and those with additional nodules on EOB-MRI after aggressive treatment (resection or radiofrequency ablation [RFA]).
Results
Among the 383 patients included, 59 had additional nodules identified using EOB-MRI. Compared with patients with solitary HCC, those with additional nodules on EOB-MRI had elevated total bilirubin, aspartate transaminase, and alanine transaminase; had a lower platelet count, higher MELD score, and highly associated with liver cirrhosis (P<0.05). Regarding long-term outcomes, 59 patients with solitary HCC and those with additional nodules after PSM were compared. Disease-free survival (DFS) and overall survival (OS) were comparable between the two groups (DFS, 60.4 vs. 44.3 months, P=0.071; OS, 82.8 vs. 84.8 months, P=0.986).
Conclusion
The aggressive treatment approach, either resection or RFA, for patients with additional nodules identified on EOBMRI was associated with long-term survival comparable with that for solitary HCC. However, further studies are required to confirm these findings.

- Treatment options for solitary hepatocellular carcinoma ≤5 cm: surgery vs. ablation: a multicenter retrospective study
- Kazuya Kariyama, Kazuhiro Nouso, Atsushi Hiraoka, Hidenori Toyoda, Toshifumi Tada, Kunihiko Tsuji, Toru Ishikawa, Takeshi Hatanaka, Ei Itobayashi, Koichi Takaguchi, Akemi Tsutsui, Atsushi Naganuma, Satoshi Yasuda, Satoru Kakizaki, Akiko Wakuta, Shohei Shiota, Masatoshi Kudo, Takashi Kumada
- J Liver Cancer. 2024;24(1):71-80. Published online November 6, 2023
- DOI: https://doi.org/10.17998/jlc.2023.09.11
- 1,131 Views
- 97 Downloads
- 3 Citations
-
Abstract
PDF
- Background/Aim
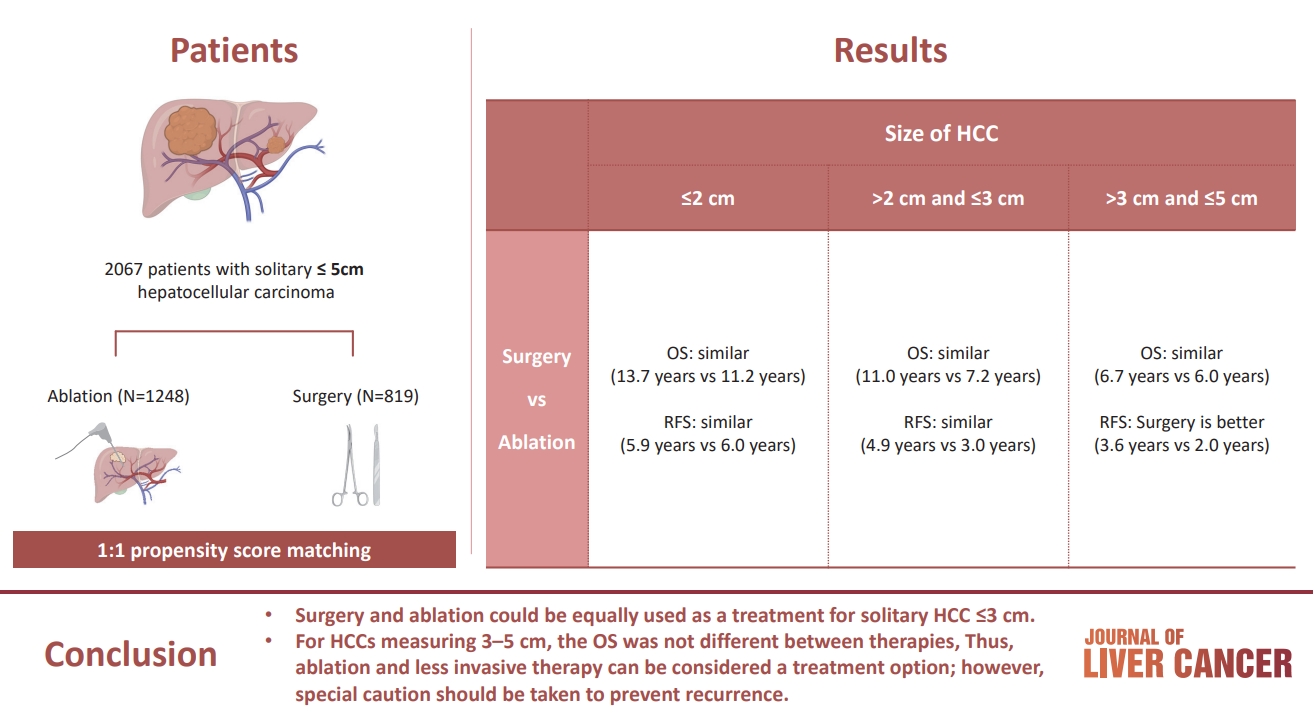
The aim of this study was to compare the therapeutic efficacy of ablation and surgery in solitary hepatocellular carcinoma (HCC) measuring ≤5 cm with a large HCC cohort database.
Methods
The study included consecutive 2,067 patients with solitary HCC who were treated with either ablation (n=1,248) or surgery (n=819). Th e patients were divided into three groups based on the tumor size and compared the outcomes of the two therapies using propensity score matching.
Results
No significant difference in recurrence-free survival (RFS) or overall survival (OS) was found between surgery and ablation groups for tumors measuring ≤2 cm or >2 cm but ≤3 cm. For tumors measuring >3 cm but ≤5 cm, RFS was significantly better with surgery than with ablation (3.6 and 2.0 years, respectively, P=0.0297). However, no significant difference in OS was found between surgery and ablation in this group (6.7 and 6.0 years, respectively, P=0.668).
Conclusion
The study suggests that surgery and ablation can be equally used as a treatment for solitary HCC no more than 3 cm in diameter. For HCCs measuring 3-5 cm, the OS was not different between therapies; thus, ablation and less invasive therapy can be considered a treatment option; however, special caution should be taken to prevent recurrence. -
Citations
Citations to this article as recorded by
- Reply to the Letter regarding “Treatment options for solitary hepatocellular carcinoma ≤5 cm: surgery vs. ablation: a multicenter retrospective study”
Kazuhiro Nouso, Kazuya Kariyama
Journal of Liver Cancer.2024; 24(1): 5. CrossRef - Radiofrequency for hepatocellular carcinoma larger than 3 cm: potential for applications in daily practice
Ji Hoon Kim, Pil Soo Sung
Journal of Liver Cancer.2024; 24(1): 1. CrossRef - Letter regarding “Treatment options for solitary hepatocellular carcinoma ≤5 cm: surgery vs. ablation: a multicenter retrospective study”
Jongman Kim
Journal of Liver Cancer.2024; 24(1): 3. CrossRef
- Reply to the Letter regarding “Treatment options for solitary hepatocellular carcinoma ≤5 cm: surgery vs. ablation: a multicenter retrospective study”
Review Article
- Management of early-stage hepatocellular carcinoma: challenges and strategies for optimal outcomes
- Jae Hyun Yoon, Sung Kyu Choi
- J Liver Cancer. 2023;23(2):300-315. Published online September 21, 2023
- DOI: https://doi.org/10.17998/jlc.2023.08.27

- 2,345 Views
- 151 Downloads
- 4 Citations
-
Abstract
PDF
- Although hepatocellular carcinoma (HCC) is associated with a poor prognosis, management of early-stage HCC is often successful with highly efficacious treatment modalities such as liver transplantation, surgical resection, and radiofrequency ablation. However, unfavorable clinical outcomes have been observed under certain circumstances, even after efficient treatment. Factors that predict unsuitable results after treatment include tumor markers, inflammatory markers, imaging findings reflecting tumor biology, specific outcome indicators for each treatment modality, liver functional reserve, and the technical feasibility of the treatment modalities. Various strategies may overcome these challenges, including the application of reinforced treatment indication criteria with predictive markers reflecting tumor biology, compensation for technical issues with up-to-date technologies, modification of treatment modalities, downstaging with locoregional therapies (such as transarterial chemotherapy or radiotherapy), and recently introduced combination immunotherapies. In this review, we discuss the challenges to achieving optimal outcomes in the management of early-stage HCC and suggest strategies to overcome these obstacles.
-
Citations
Citations to this article as recorded by- Diosgenin potentiates the anticancer effect of doxorubicin and volasertib via regulating polo-like kinase 1 and triggering apoptosis in hepatocellular carcinoma cells
Eman H. Yousef, Mohamed E. El-Mesery, Maha R. Habeeb, Laila A. Eissa
Naunyn-Schmiedeberg's Archives of Pharmacology.2024;[Epub] CrossRef - Comparison of Surgical Resection and Radiofrequency Ablation in Elderly Patients with Hepatocellular Carcinoma
Jun Il Kim, Jayoun Lee, Gi Hong Choi, Min Woo Lee, Dong Ah Park, Jeong-Ju Yoo
Digestive Diseases and Sciences.2024; 69(3): 1055. CrossRef - Radiofrequency for hepatocellular carcinoma larger than 3 cm: potential for applications in daily practice
Ji Hoon Kim, Pil Soo Sung
Journal of Liver Cancer.2024; 24(1): 1. CrossRef - Efficacy of Transarterial Chemoembolization (TACE) for Early-Stage Hepatocellular Carcinoma
Moonhyung Lee, Hyun Phil Shin
Medicina.2023; 59(12): 2174. CrossRef
- Diosgenin potentiates the anticancer effect of doxorubicin and volasertib via regulating polo-like kinase 1 and triggering apoptosis in hepatocellular carcinoma cells
Original Article
- The efficacy of treatment for hepatocellular carcinoma in elderly patients
- Han Ah Lee, Sangheun Lee, Hae Lim Lee, Jeong Eun Song, Dong Hyeon Lee, Sojung Han, Ju Hyun Shim, Bo Hyun Kim, Jong Young Choi, Hyunchul Rhim, Do Young Kim
- J Liver Cancer. 2023;23(2):362-376. Published online September 14, 2023
- DOI: https://doi.org/10.17998/jlc.2023.08.03

- 1,360 Views
- 72 Downloads
-
Abstract
PDF
 Supplementary Material
Supplementary Material - Background/Aim
Despite the increasing proportion of elderly patients with hepatocellular carcinoma (HCC) over time, treatment efficacy in this population is not well established.
Methods
Data collected from the Korean Primary Liver Cancer Registry, a representative cohort of patients newly diagnosed with HCC in Korea between 2008 and 2017, were analyzed. Overall survival (OS) according to tumor stage and treatment modality was compared between elderly and non-elderly patients with HCC.
Results
Among 15,186 study patients, 5,829 (38.4%) were elderly. A larger proportion of elderly patients did not receive any treatment for HCC than non-elderly patients (25.2% vs. 16.7%). However, OS was significantly better in elderly patients who received treatment compared to those who did not (median, 38.6 vs. 22.3 months; P<0.001). In early-stage HCC, surgery yielded significantly lower OS in elderly patients compared to non-elderly patients (median, 97.4 vs. 138.0 months; P<0.001), however, local ablation (median, 82.2 vs. 105.5 months) and transarterial therapy (median, 42.6 vs. 56.9 months) each provided comparable OS between the two groups after inverse probability of treatment weighting (IPTW) analysis (all P>0.05). After IPTW, in intermediate-stage HCC, surgery (median, 66.0 vs. 90.3 months) and transarterial therapy (median, 36.5 vs. 37.2 months), and in advanced-stage HCC, transarterial (median, 25.3 vs. 26.3 months) and systemic therapy (median, 25.3 vs. 26.3 months) yielded comparable OS between the elderly and non-elderly HCC patients (all P>0.05).
Conclusions
Personalized treatments tailored to individual patients can improve the prognosis of elderly patients with HCC to a level comparable to that of non-elderly patients.
Case Report
- Complete response to local therapy for advanced hepatocellular carcinoma with lung metastasis: a case report
- Daeun Kim, Seiyeon Park, Won Sohn, Hyun Pyo Hong, Byung Ik Kim
- J Liver Cancer. 2022;22(1):51-56. Published online January 27, 2022
- DOI: https://doi.org/10.17998/jlc.2021.12.28

- 3,147 Views
- 97 Downloads
-
Abstract
PDF
- The concept of oligometastasis is widely accepted for various types of solid tumors; accordingly, better outcomes can be anticipated with aggressive local interventions. The treatment of advanced hepatocellular carcinoma (HCC) with extrahepatic metastasis is systemic therapy. However, treatment responses to systemic therapy are poor. Recently, a small number of metastatic cancers (oligometastasis) have been controlled by local therapy rather than systemic therapy. Our study reports a case of a 66-year-old male patient with advanced HCC with lung metastasis, which was treated with local therapy. There were less than four metastases in the lungs, which were treated with wedge resection, radiofrequency, and radiation therapy. He repeatedly underwent local therapy for lung oligometastasis and locoregional therapy for intrahepatic HCC rather than systemic therapy; control by local therapy was possible as his liver function was preserved with Child-Turcotte-Pugh class A.
Original Articles
- The effect of nucleos(t)ide analogues on clinical outcomes of patients treated with transarterial chemoembolization and radiofrequency ablation for hepatitis B virus-related hepatocellular carcinoma
- Jae Min Park, Won Hyeok Choe, Jeong Han Kim, So Young Kwon, Byung Chul Yoo
- J Liver Cancer. 2021;21(2):155-162. Published online September 30, 2021
- DOI: https://doi.org/10.17998/jlc.2021.09.22
- 3,391 Views
- 92 Downloads
- 3 Citations
-
Abstract
PDFSupplementary Material
- Background/Aims
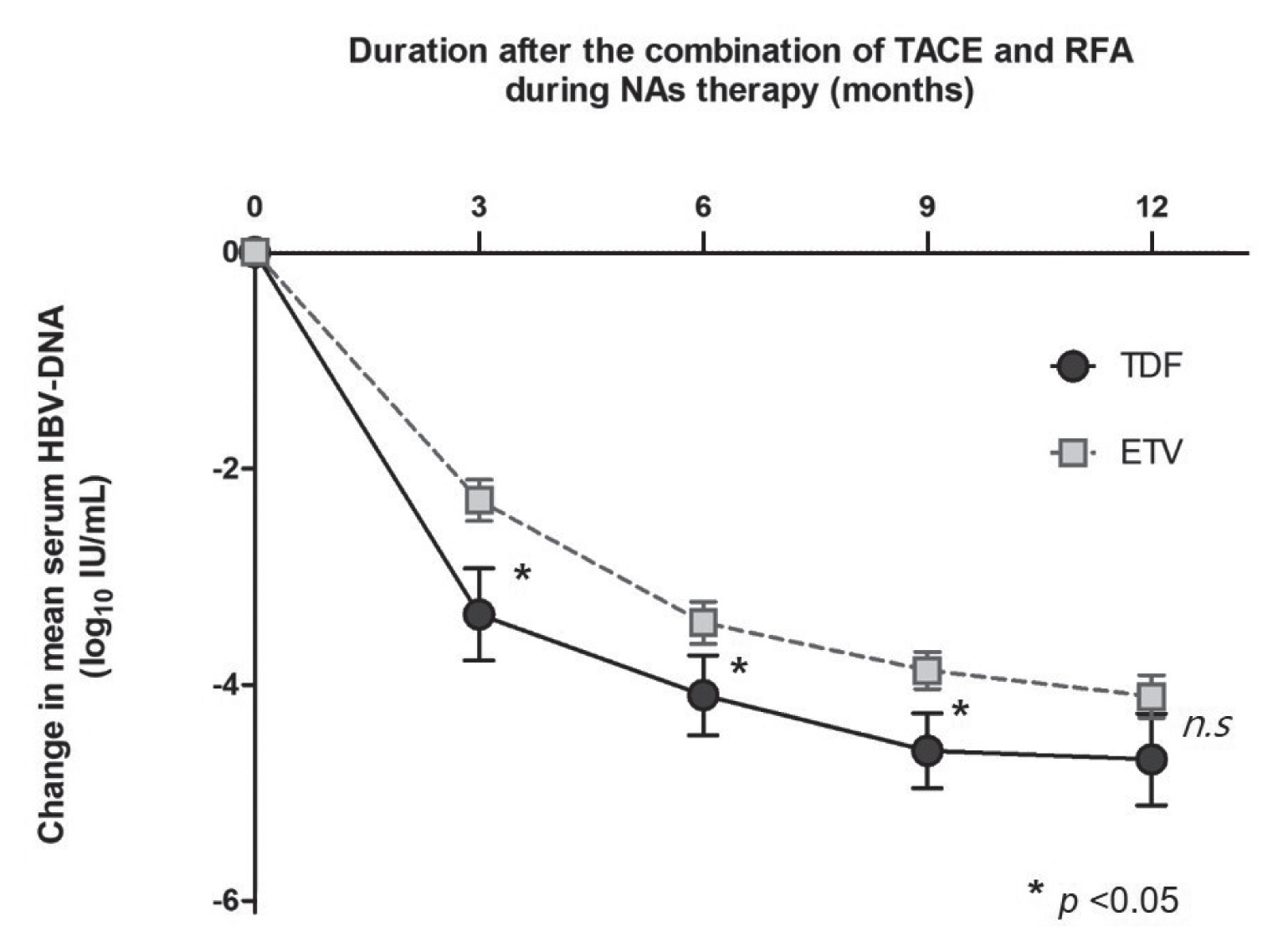
Because hepatitis B virus (HBV) replication has been known to play an important role in cancer recurrence after curative treatment of HBV-related hepatocellular carcinoma (HCC), we examined whether treatment based on nucleos(t)ide analogues (NAs) might decrease the recurrence rate and improve patient survival.
Methods
The retrospective cohort study enrolled 73 patients with chronic hepatitis B who were treated with transarterial chemoembolization (TACE) and radiofrequency ablation (RFA) with curative intent for HCC. Among those, 30 and 43 patients were treated with tenofovir disoproxil fumarate (TDF) and entecavir (ETV), respectively.
Results
Of the 73 patients, 51 experienced HCC recurrence, and 14 patients were dead during a follow-up of 73±34 months. Multivariate analyses showed that tumor size (hazard ratio [HR], 1.590; 95% confidence-interval [CI], 1.106-2.285; P=0.012) and Child-Pugh class B (vs. class A/non cirrhosis; HR, 5.794; 95% CI, 2.311-14.523; P=0.001) was significantly associated with HCC recurrence, and Child-Pugh class B (HR, 7.357; 95% CI, 2.100-25.777; P=0.002) was an independent unfavorable prognostic factor for survival. During NAs therapy, TDF was superior to ETV for complete viral response at 1 year after the date of combination of TACE and RFA (P=0.016). However, the risks of HCC recurrence and survival were not significantly different between those treated with TDF versus ETV.
Conclusions
TDF was superior to ETV for achieving complete viral response. However, the recurrence and mortality after TACE and RFA for HBV-related HCC were not significantly different between patients treated with TDF versus ETV. -
Citations
Citations to this article as recorded by- Enhanced prognosis of HCC patients undergoing radical treatments with tenofovir versus entecavir: A meta-analysis based on propensity score matching studies
Qingyan Kong, Mengshi Yi, Fei Teng, Zheyu Chen
Asian Journal of Surgery.2024; 47(1): 55. CrossRef - Tenofovir versus entecavir on the prognosis of hepatitis B virus-related hepatocellular carcinoma: a systematic review and meta-analysis
Hui Liu, Cheng-Long Han, Bao-Wen Tian, Zi-Niu Ding, Ya-Fei Yang, Yun-Long Ma, Chun-Cheng Yang, Guang-Xiao Meng, Jun-Shuai Xue, Dong-Xu Wang, Zhao-Ru Dong, Zhi-Qiang Chen, Jian-Guo Hong, Tao Li
Expert Review of Gastroenterology & Hepatology.2023; 17(6): 623. CrossRef - A nationwide study on the current treatment status and natural prognosis of hepatocellular carcinoma in elderly
Jeong-Ju Yoo, Jayoun Lee, Gi Hong Choi, Min Woo Lee, Dong Ah Park
Scientific Reports.2023;[Epub] CrossRef
- Enhanced prognosis of HCC patients undergoing radical treatments with tenofovir versus entecavir: A meta-analysis based on propensity score matching studies
- Transarterial chemoembolization using drug-eluting bead compared with radiofrequency ablation for treatment of single small hepatocellular carcinoma: a pilot non-randomized trial
- Tae Hoon Kim, Na Hye Kim, Jin Dong Kim, Young Nam Kim, Yu Jin Kim, Eun Jung Kim, Ki Deok Yoo, Choong Heon Ryu, Ha Hun Song, Hyun Kim
- J Liver Cancer. 2021;21(2):146-154. Published online August 11, 2021
- DOI: https://doi.org/10.17998/jlc.2021.05.20

- 4,428 Views
- 138 Downloads
- 3 Citations
-
Abstract
PDFSupplementary Material
- Background/Aims
Surgical resection, transplantation, and radiofrequency ablation (RFA) are generally accepted as amenable treatments for small hepatocellular carcinoma (HCC). Recently drug-eluting beads (DEB) which had several treatment advantages were introduced for transarterial chemoembolization (TACE). The aim of this study was to evaluate feasibility and safety of DEB-TACE compared with RFA for the treatment of single small HCC.
Methods
In this pilot non-randomized trial, we assessed retrospective data of 40 patients who underwent DEB-TACE (n=21) or RFA (n=19) for single small (≤3 centimeter in greatest dimension) HCC. The primary outcomes were tumor response and time to recurrence. The secondary outcome was treatment-related complications.
Results
Complete response rate to DEB-TACE and RFA after first follow-up assessment was 90.5% and 94.7%, respectively (P=1.000). During mean follow-up of 87.6 months (95% confidence interval: 74.4-102), 7 patients experienced local recurrence. The 6- and 12-month cumulative local recurrence rate was 5.0% and 21.8% in DEB-TACE vs. 11.1% and 17.0% in RFA group (P=0.877). A total 14 distant intrahepatic recurrences were developed and 12- and 24-month cumulative distant intrahepatic recurrence rate was 20.6% and 42.7% in DEBTACE vs. 17.2% and 36.3% in RFA group (P=0.844). Two patients experienced gangrenous cholecystitis after DEB-TACE requiring cholecystectomy as treatment-related adverse event.
Conclusions
Tumor response and recurrence rate after single session of DEB-TACE or RFA were similar. DEB-TACE could be applied selectively in patients with a single small HCC if the other therapeutic modality is unfeasible. -
Citations
Citations to this article as recorded by- Incidence and Risk Factors of Acute Ischemic Cholecystitis after Transarterial Chemoembolization: Correlation with Cone Beam CT Findings
Jong Yeong Kim, Jung Suk Oh, Ho Jong Chun, Su Ho Kim
Journal of the Korean Society of Radiology.2024; 85(2): 363. CrossRef - Drug-Eluting Bead Transarterial Chemoembolization Versus Radiofrequency Ablation as an Initial Treatment of Single Small (≤ 3 cm) Hepatocellular Carcinoma
Somin Lee, Yong Yeon Jeong, Byung Chan Lee, Sang Soo Shin, Suk Hee Heo, Hyoung Ook Kim, Chan Park, Won Gi Jeong
Journal of Korean Medical Science.2023;[Epub] CrossRef - Comparable Outcomes in Early Hepatocellular Carcinomas Treated with Trans-Arterial Chemoembolization and Radiofrequency Ablation
Benjamin Wei Rong Tay, Daniel Q. Huang, Muthiah Mark, Neo Wee Thong, Lee Guan Huei, Lim Seng Gee, Low How Cheng, Lee Yin Mei, Prem Thurairajah, Lim Jia Chen, Cheng Han Ng, Wen Hui Lim, Darren Jun Hao Tan, Da Costa Maureen, Kow Wei Chieh Alfred, Iyer Shrid
Biomedicines.2022; 10(10): 2361. CrossRef
- Incidence and Risk Factors of Acute Ischemic Cholecystitis after Transarterial Chemoembolization: Correlation with Cone Beam CT Findings
Case Reports
- Gallbladder Fistula Treated with N-Butyl-2-Cyanoacrylate after Radiofrequency Ablation in a Hepatocellular Carcinoma Patient: a Case Report
- In Tae So, Byoung Kook Jang, Jae Seok Hwang, Young hwan Kim
- J Liver Cancer. 2019;19(1):69-73. Published online March 31, 2019
- DOI: https://doi.org/10.17998/jlc.19.1.69

- 3,658 Views
- 55 Downloads
-
Abstract
PDF
- Radiofrequency ablation (RFA) is a minimally invasive local therapy for hepatocellular carcinoma (HCC). Even though RFA is considered to be a safe treatment modality, a variety of complications have been reported. Recently, we encountered a case of refractory fistula between a liver abscess and the gallbladder after RFA. A 64-year-old woman diagnosed with HCC associated with chronic hepatitis B was treated by RFA. After RFA, she experienced abdominal pain, and abdominal computed tomography (CT) revealed a liver abscess complicated by a previous treatment of HCC, she was treated with intravenous antibiotics and percutaneous abscess drainage. Follow-up abdominal CT revealed a fistula between the liver abscess and gallbladder, which was successfully treated with percutaneous transcatheter n-butyl-2-cyanoacrylate (NBCA) embolization. We herein report the rare case of a refractory fistula between a liver abscess and the gallbladder after RFA in a patient treated with NBCA embolization.
- Needle-tract Seeding of Hepatocellular Carcinoma at Chest Wall: A Report of Two Cases
- Kim, Dae Jung , Kim, Gwangil
- J Liver Cancer. 2018;18(1):63-66. Published online March 31, 2018
- DOI: https://doi.org/10.17998/jlc.18.1.63
- 1,462 Views
- 24 Downloads
-
Abstract
PDF
- We report two cases of needle-tract seeding after cryoablation and radiofrequency ablation for hepatocellular carcinomas. The seeding nodule appeared 6 and 12 months on the follow-up computed tomographic scan, respectively. In both cases, the seeding nodules were solitary in the chest wall, and could be completely resected.
Review Articles
- The Role of Combination of Transarterial Chemoebolization and Radiofrequency Ablation for Hepatocellular Carcinoma Treatment
- Byoung Kuk Jang
- J Liver Cancer. 2017;17(1):15-18. Published online March 31, 2017
- DOI: https://doi.org/10.17998/jlc.17.1.15
- 1,343 Views
- 24 Downloads
-
Abstract
PDF
- Recently, various combination therapies have been applied to the treatment of hepatocellular carcinoma (HCC). Among various treatment modalities, transarterial chemoembolization (TACE) and radiofrequency ablation (RFA) were combined to improve the therapeutic effect of RFA. The decrease of blood flow by TACE can increase the size of the ablation area by reducing heat loss during RFA. Based on these theoretical advantages, TACE and RFA combination therapy have been tried for the treatment of patients with HCC which is not feasible to be removed by surgery. However, TACE and RFA combination therapy has not been standardized by various protocols for each study. This review discusses the implications and role of this treatment, although there are several limitations to clearly demonstrate the indications and efficacy of TACE and RFA combination therapies.
- Radiofrequency Ablation for Hepatocellular Carcinoma
- Se Young Jang, So Young Park
- J Liver Cancer. 2015;15(2):79-83. Published online September 30, 2015
- DOI: https://doi.org/10.17998/jlc.15.2.79
- 1,053 Views
- 18 Downloads
-
Abstract
PDF
- Radiofrequency ablation (RFA) takes an important role in management of hepatocellular carcinoma (HCC) as the most popular local therapy in the world. There are many data supporting that RFA is an excellent treatment modality for early-stage HCC with favorable treatment outcomes and minimal invasiveness. Currently, RFA extends treatement indications from unresectable early-stage HCC to intermediate-stage HCC in selected cases. Thus, with technical advances in guidance and ablation as well as devices, RFA widens its territory in the combat field against HCC. (J Liver Cancer 2015;15:79-83)
- New Techniques of Ultrasound-guided Radiofrequency Ablation for Hepatocellular Carcinoma
- Min Woo Lee
- J Liver Cancer. 2014;14(2):89-96. Published online September 30, 2014
- DOI: https://doi.org/10.17998/jlc.14.2.89
- 947 Views
- 10 Downloads
-
Abstract
PDF
- In Korea, radiofrequency ablation (RFA) of hepatocellular carcinoma (HCC) is most widely used under ultrasonography (US) guidance. With the technical development, small HCCs in challenging locations can be ablated effectively. Both fusion imaging and contrast-enhanced US is useful for identifying small inconspicuous HCCs on conventional US, thereby enable us to conduct successful RFA. Artificial ascites can enhance ultrasonic window and is helpful in avoiding thermal injury to the surrounding organs. Laparoscopy is also useful for guidance of RFA for subcapsular HCCs which are difficult to approach percutaneously. (J Liver Cancer 2014;14:89-96)
Case Reports
- Clinical Outcome of Completely Ablated Hepatocellular Carcinoma in Single Session in Patients with Decompensated Liver Cirrhosis
- Min Seon Park, Soon Ho Um, Ho Sang Ryu, Yeon Seok Seo, Sun Young Yim, Chang Ho Jung, Tae Hyung Kim, Dae Hoe Gu
- J Liver Cancer. 2014;14(2):139-142. Published online September 30, 2014
- DOI: https://doi.org/10.17998/jlc.14.2.139
- 985 Views
- 2 Downloads
-
Abstract
PDF
- Most cases of hepatocellular carcinoma (HCC) occur in the Asia-Pacific region and in patients with underlying hepatitis B and C viral infection. Although surgical resection is the gold standard for treatment of HCC, only a few patients are surgical candidates because of their lack of hepatic reserve. Liver transplantation, which eradicates HCC and replaces damaged noncancerous hepatic parenchyma, is regarded as the best treatment for HCC in patients with decompensated liver cirrhosis. However, the shortage of donors limit its widespread use. Furthermore, the long waiting time for liver transplantation allow for tumor progression and reduce patient survival. Given this long wait, there is a reasonable clinical need in the meantime for minimally invasive methods to avoid progression of HCC in patients with decompensated liver cirrhosis. We herein offer our experiences of therapeutic efficacy and complications of the procedure and the changes in liver function before and after TACE and radiofrequency ablation in patients with HCC and decompensated liver cirrhosis, defined as a Child-Pugh-Turcotte score above 7. (J Liver Cancer 2014;14:139-142)
- A Case of Hepatocellular Carcinoma with Improved Decompansated Liver Cirrhosis with Combination Treatment of Transarterial Chemoembolization and Radiofrequency Ablation
- Hyung Min Yu, Won Hyeok Choe, So Young Kwon, Jeong Han Kim
- J Liver Cancer. 2014;14(2):131-134. Published online September 30, 2014
- DOI: https://doi.org/10.17998/jlc.14.2.131
- 1,092 Views
- 5 Downloads
-
Abstract
PDF
- A 54-year-old female patient with no medical history visited our hospital complaining of both pretibial pitting oedema for 6 months, and abdominal distension for 1 month. Computed tomography and magnetic resonance imaging revealed an 2.3cm sized tumour at segment 2 of the liver. Her Child-Turcotte-Pugh (CTP) class was C (score 11) at the initial visit. She was diagnosed as hepatocellular carcinoma (UICC stage II, BCLC stage D), and then she underwent conservative treatment for 1 month. After one month of conservative treatment, her liver function was improved to CTP class B (score 8), and then she underwent combination treatment of transarterial chemoembolization and radiofrequency ablation. However, her liver function was deteriorated gradually. She was transferred to other hospital for liver transplantation eventually. (J Liver Cancer 2014;14:131-134)
- A Case of Successful Treatment by Radiofrequency Ablation for Pulmonary Metastasis of Hepatocellular Carcinoma
- Jae Chan Park, Yun Soo Kim, Young Kul Jung, Myung Hee Kang, Oh Sang Kwon, Duck Joo Choi, Yang Suh Ku, Ju Hyun Kim
- Journal of the Korean Liver Cancer Study Group. 2013;13(1):51-56. Published online February 28, 2013
- DOI: https://doi.org/10.17998/jlc.13.1.51
- 3,682 Views
- 7 Downloads
-
Abstract
PDF
- Surgical resection or liver transplantation is a main curative modality for hepatocellular carcinoma (HCC). But nowadays local ablation therapy is being accepted as a useful option for local control therapy for HCC. Here we present a case of 59 years old male with hepatitis B virus related liver cirrhosis, who underwent surgery for HCC at S6 two years ago. He had received percutaneous ethanol injection (PEI), radiofrequency ablation (RFA) and multiple sessions of transarterial chemoembolization (TACE) for intrahepatic recurrences of HCC after surgery. A small radio-opaque lesion occurred at the left upper lobe of lung. Metastatic HCC was confirmed by CT-guided percutaneous needle core biopsy. CT-guided RFA for pulmonary metastasis was performed. Now it is been 11 months after the treatment without any recurrence.
 First
First Prev
Prev


 Follow JLC on Twitter
Follow JLC on Twitter