 E-submission
E-submission
Search
- Page Path
- HOME > Search
Case Report
- Metastatic papillary renal cell carcinoma with portal vein tumor thrombosis confirmed on blind liver biopsy
- Hun Kim, Tae Hoon Roh, Jun Seop Lee, Min Seong Kim, Beom Kyung Kim
- J Liver Cancer. 2024;24(1):113-117. Published online November 29, 2023
- DOI: https://doi.org/10.17998/jlc.2023.11.05

- 911 Views
- 82 Downloads
-
 Abstract
Abstract
 PDF
PDF - Portal vein tumor thrombosis (PVTT) is an uncommon condition in which tumor cells expand into the vessels, causing blood clot formation in the portal vein. PVTT is mainly associated with hepatocellular carcinoma, leading to an unfavorable prognosis; however, it can also develop in patients with other cancer types. Herein, we report a case of metastatic renal cell carcinoma diagnosed by a blind liver biopsy in a patient with dynamic computed tomography-confirmed portal vein thrombosis and cholangiopathy. This case illustrates the importance of systematic surveillance with routine laboratory tests and contrast-enhanced imaging studies on patients with cancer to detect potential liver infiltration of metastatic cancer.

Original Article
- Use of doxorubicin-eluting bead transarterial chemoembolization for unresectable hepatocellular carcinoma with portal vein invasion: a prospective study
- Su Jong Yu, Yun Bin Lee, Eun Ju Cho, Jeong-Hoon Lee, Hyo-Cheol Kim, Jin Wook Chung, Jung-Hwan Yoon, Yoon Jun Kim
- J Liver Cancer. 2023;23(1):166-176. Published online March 3, 2023
- DOI: https://doi.org/10.17998/jlc.2023.02.08
- 2,150 Views
- 98 Downloads
-
Abstract
PDF
 Supplementary Material
Supplementary Material - Background/Aim
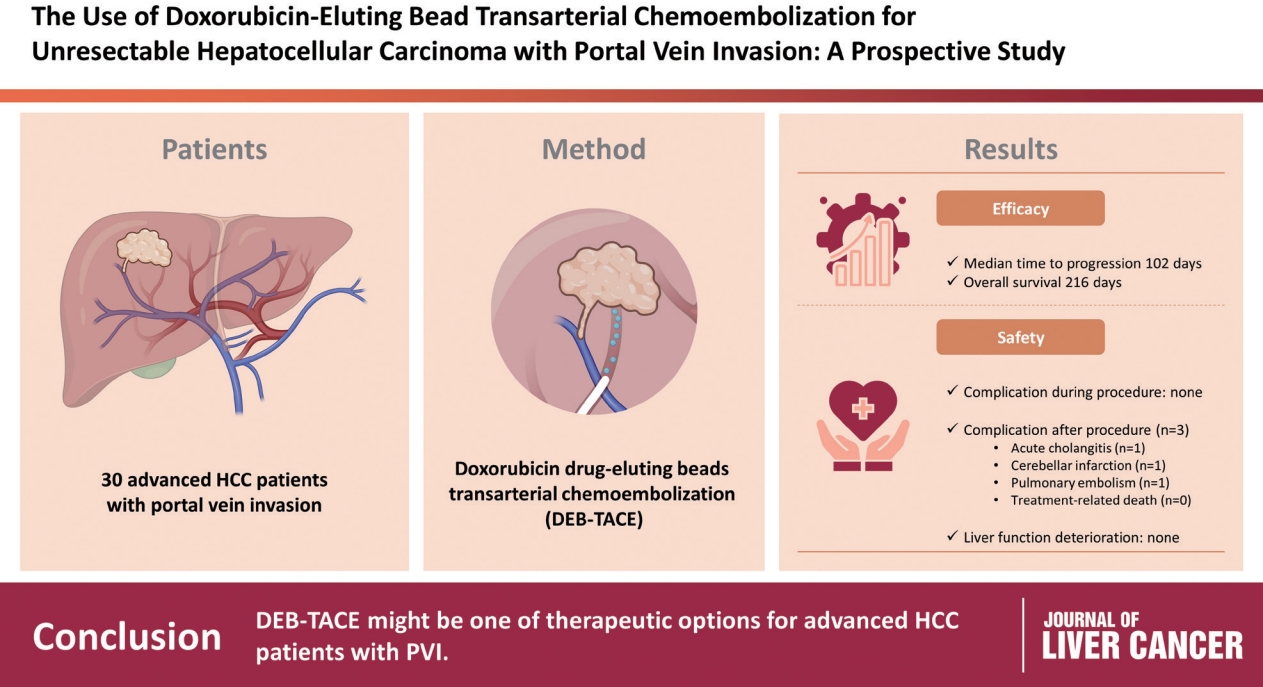
To evaluate the applicability of transarterial chemoembolization (TACE) treatment with doxorubicin drug-eluting beads (DEBs) in advanced hepatocellular carcinoma (HCC) patients with portal vein invasion (PVI).
Methods
This prospective study was approved by the institutional review board and informed consent was obtained from all participants. A total of 30 HCC patients with PVI received DEB-TACE between 2015 and 2018. The following parameters were evaluated: complications during DEB-TACE, abdominal pain, fever, and laboratory outcomes, including liver function change. Overall survival (OS), time to progression (TTP), and adverse events were also analyzed and assessed.
Results
DEBs measuring 100–300 μm in diameter were loaded with doxorubicin (150 mg per procedure). There were no complications during DEB-TACE and no significant differences in the levels of prothrombin time, serum albumin, or total bilirubin at follow-up compared to baseline. The median TTP was 102 days (95% confidence interval [CI], 42–207 days) and the median OS was 216 days (95% CI, 160–336 days). Three patients (10%) had severe adverse reactions, including transient acute cholangitis (n=1), cerebellar infarction (n=1), and pulmonary embolism (n=1), but no treatment-related death occurred.
Conclusions
DEB-TACE may be a therapeutic option for advanced HCC patients with PVI.
Case Report
- Long-term survival after CCRT and HAIC followed by ALPPS for hepatocellular carcinoma with portal vein invasion: a case report
- In-Jung Kim, Sung Hwan Yoo, Jung Il Lee, Kwan Sik Lee, Hyun Woong Lee, Jin Hong Lim
- J Liver Cancer. 2022;22(1):84-90. Published online March 22, 2022
- DOI: https://doi.org/10.17998/jlc.2022.03.07
- 2,824 Views
- 71 Downloads
- 1 Citation
-
Abstract
PDF
- There are various methods for treating advanced hepatocellular carcinoma with portal vein invasion, such as systemic chemotherapy, transarterial chemoembolization, transarterial radioembolization, and concurrent chemoradiotherapy. These methods have similar clinical efficacy but are designed with a palliative aim. Herein, we report a case that experienced complete remission through “associating liver partition and portal vein ligation for staged hepatectomy (ALPPS)” after concurrent chemoradiotherapy and hepatic artery infusion chemotherapy. In this patient, concurrent chemoradiotherapy and hepatic artery infusion chemotherapy induced substantial tumor shrinkage, and hypertrophy of the nontumor liver was sufficiently induced by portal vein ligation (stage 1 surgery) followed by curative resection (stage 2 surgery). Using this approach, long-term survival with no evidence of recurrence was achieved at 16 months. Therefore, the optimal use of ALPPS requires sufficient consideration in cases of significant hepatocellular carcinoma shrinkage for curative purposes.
-
Citations
Citations to this article as recorded by
- Is multidisciplinary treatment effective for hepatocellular carcinoma with portal vein tumor thrombus?
Won Hyeok Choe
Journal of Liver Cancer.2022; 22(1): 1. CrossRef
- Is multidisciplinary treatment effective for hepatocellular carcinoma with portal vein tumor thrombus?
Review Article
- Liver transplantation for hepatocellular carcinoma with portal vein tumor thrombosis
- Sang Jin Kim, Jong Man Kim
- J Liver Cancer. 2021;21(2):105-112. Published online September 2, 2021
- DOI: https://doi.org/10.17998/jlc.2021.03.17

- 5,063 Views
- 222 Downloads
- 3 Citations
-
Abstract
PDF
- Traditionally, liver transplantation for hepatocellular carcinoma with portal vein tumor thrombosis is not recommended. However, with recent developments in locoregional therapies for hepatocellular carcinoma, more aggressive treatments have been attempted for advanced hepatocellular carcinoma. Recently, various studies on locoregional therapies for downstaging followed by living donor liver transplantation reported inspiring overall survival and recurrence-free survival of patients. These downstaging procedures included three-dimensional conformal radiation therapy, trans-arterial chemoembolization, stereotactic body radiation therapy, trans-arterial radioembolization, hepatic arterial infusion chemotherapy and combinations of these therapies. Selection of the optimal downstaging protocol should depend on tumor location, biology and background liver status. The risk factors affecting outcome include pre-downstaging alpha-fetoprotein values, delta alpha-fetoprotein values, disappearance of portal vein tumor thrombosis on imaging and meeting the Milan criteria or not after downstaging. For hepatocellular carcinoma with portal vein tumor thrombosis, downstaging procedure with liver transplantation in mind would be helpful. If the reaction of the downstaged tumor is good, liver transplantation may be performed.
-
Citations
Citations to this article as recorded by- Metastatic papillary renal cell carcinoma with portal vein tumor thrombosis confirmed on blind liver biopsy
Hun Kim, Tae Hoon Roh, Jun Seop Lee, Min Seong Kim, Beom Kyung Kim
Journal of Liver Cancer.2024; 24(1): 113. CrossRef - Refining MRI-based criteria for portal vein invasion in hepatocellular carcinoma: improving sensitivity beyond portal vein tumor thrombosis
Jeongju Kim, Woo Kyoung Jeong, Jong Man Kim, Sang Yun Ha, Kyunga Kim
Abdominal Radiology.2023; 49(2): 437. CrossRef - Prediction models of hepatocellular carcinoma recurrence after liver transplantation: A comprehensive review
Sang Jin Kim, Jong Man Kim
Clinical and Molecular Hepatology.2022; 28(4): 739. CrossRef
- Metastatic papillary renal cell carcinoma with portal vein tumor thrombosis confirmed on blind liver biopsy
Original Article
- Multicenter Planning Comparison of Stereotactic Body Radiotherapy for Hepatocellular Carcinoma with Major Portal Vein Tumor Thrombosis (KROG 16-17)
- Bae, Sun Hyun , Kim, Mi Sook , Jang, Won Il , Kim, Jin Ho , Kim, Woo Chul , Kim, Jin Hee , Jeong, Bae Kwon , Kim, Yong Ho , Jo, Sunmi , Choi, Chul Won , Park, Younghee , Cho, Kwang Hwan
- J Liver Cancer. 2018;18(2):130-141. Published online September 30, 2018
- DOI: https://doi.org/10.17998/jlc.18.2.130
- 3,957 Views
- 54 Downloads
- 1 Citation
-
Abstract
PDF
- Background/Aims
To evaluate the technical feasibility of stereotactic body radiotherapy (SBRT) for hepatocellular carcinoma (HCC) with the major portal vein tumor thrombosis (PVTT).
Methods
Ten institutions affiliated with the Korean Stereotactic Radiosurgery Group were provided the contours of four cases: the first case was the first branch PVTT with sufficient normal liver volume (NLV), the second was the first branch PVTT with insufficient NLV, the third was the main trunk PVTT at confluence level, and the fourth was the main trunk PVTT with entire length. The institutions were asked to make SBRT plans according to their current treatment protocols and to complete facility questionnaires.
Results
Based on institutional protocols, SBRT was feasible in nine institutions for the first case (32-60 Gy in 3-5 fractions), in eight institutions for the second case (32-50 Gy in 3-5 fractions), in seven institutions for the third case (35-60 Gy in 3-5 fractions), and in four institutions for the fourth case (35-42 Gy in 4-5 fractions). The other institutions recommended hypo- or conventional fractionation due to insufficient NLV or gastrointestinal organ proximity. With analysis of the SBRT dose to the central hepatobiliary tract, the major PVTT could theoretically be associated with a high risk of hepatobiliary toxicity.
Conclusions
Although SBRT is a technically feasible option for HCC with the major PVTT, there was a variability among the participating institutions. Therefore, further studies will be necessary to standardize the practice of SBRT for the major PVTT. -
Citations
Citations to this article as recorded by- Current status of stereotactic body radiotherapy for the treatment of hepatocellular carcinoma
Jongmoo Park, Jae Won Park, Min Kyu Kang
Yeungnam University Journal of Medicine.2019; 36(3): 192. CrossRef
- Current status of stereotactic body radiotherapy for the treatment of hepatocellular carcinoma
Case Report
- A Case of Complete Response with Biliary Stenosis after Hepatic Arterial Injection and Stereotactic Body Radiotherapy to Hepatoecllular Carcinoma with Portal Vein Thrombosis
- Rim, Chai Hong , Im, Hyung Joon , Jung, Young Geol , Chung, Hwan Hoon , Seo, Sang Joon , Yoon, Won Sup
- J Liver Cancer. 2018;18(1):75-79. Published online March 31, 2018
- DOI: https://doi.org/10.17998/jlc.18.1.75
- 2,021 Views
- 36 Downloads
-
Abstract
PDF
- Curative treatment of hepatocellular carcinoma (HCC) with portal vein invasion is difficult to achieve, and the prognosis is dismal. Combining external beam radiotherapy (EBRT) with hepatic arterial infusion chemotherapy (HAIC) has shown favorable local therapeutic effects for patients with HCC exhibiting portal vein invasion. Stereotactic body radiotherapy (SBRT) is a recently developed EBRT modality that shows excellent tumor control. The combination of SBRT and HAIC for HCC with portal vein invasion has not been well-studied. We report a patient with HCC and portal vein invasion who achieved 15 months of survival with complete response status after combination SBRT and HAIC. The patient later experienced grade 3 biliary stricture and died of liver abscesses of unknown etiologies that subsequently appeared.
Original Article
- Factors Affecting Prognosis of Hepatocellular Carcinoma with Portal Vein Tumor Thrombosis: Implications for Future Therapeutic Strategies
- Sang Jun Suh, Hyung Joon Yim, Dong Won Lee, Jong Jin Hyun, Young Kul Jung, Ji Hoon Kim, Yeon Seok Seo, Jong Eun Yeon, Kwan Soo Byun, Soon Ho Um
- J Liver Cancer. 2017;17(1):60-71. Published online March 31, 2017
- DOI: https://doi.org/10.17998/jlc.17.1.60
- 2,147 Views
- 23 Downloads
- 1 Citation
-
Abstract
PDF
- Background/Aims
Hepatocellular carcinoma (HCC) with portal vein tumor thrombosis (PVTT) exhibits poor prognosis. The aim of this study is to evaluate factors associated with survival of HCC patients with PVTT to suggest better therapeutic options.
Methods
Patients with HCC which were newly diagnosed at three tertiary hospitals between January 2004 and December 2012, were reviewed retrospectively. Among them, Barcelona Clinic of Liver Cancer stage C patients with PVTT were identified. Factors affecting overall survival (OS) were analyzed and efficacies of the treatment modalities were compared.
Results
Four hundred sixty five patients with HCC and PVTT were included. Liver function, tumor burden, presence of extrahepatic tumor, alfa fetoprotein, and treatment modalities were significant factors associated with OS. Treatment outcomes were different according to the initial modalities. OS of the patients who received hepatic resection, radiofrequency ablation (RFA), transarterial chemoembolization (TACE), hepatic arterial infusion chemotherapy (HAIC), sorafenib, systemic cytotoxic chemotherapy, radiation therapy (without combination), and supportive care were 27.8, 7.1, 6.7, 5.3, 2.5, 3.0, 1.8, and 0.9 months, respectively (P<0.001). Curative-intent treatments such as hepatic resection or RFA were superior to noncurativeintent treatments (P<0.001). TACE or HAIC was superior to sorafenib or systemic chemotherapy (P<0.001). Combining radiotherapy to TACE or HAIC did not provide additional benefit on OS (P=0.096).
Conclusions
Treatment modalities as well as baseline factors significantly influenced on OS of HCC patients with PVTT. Whenever possible, curative intent treatments should be preferentially considered. If unable, locoregional therapy would be a better choice than systemic therapy in HCC patients with PVTT. -
Citations
Citations to this article as recorded by- Value of surgical resection compared to transarterial chemoembolization in the treatment of hepatocellular carcinoma with portal vein tumor thrombus: A meta-analysis of hazard ratios from five observational studies
Keera Kang, Sung Kyu Song, Chul-Woon Chung, Yongkeun Park
Annals of Hepato-Biliary-Pancreatic Surgery.2020; 24(3): 243. CrossRef
- Value of surgical resection compared to transarterial chemoembolization in the treatment of hepatocellular carcinoma with portal vein tumor thrombus: A meta-analysis of hazard ratios from five observational studies
Review Article
- Locoregional Treatment of Hepatocellular Carcinoma with Portal Vein Tumor Thrombosis
- Sang Youn Hwang, Ryoung-Go Kim, Cheol-Won Choi, Sang Bu Ahn
- J Liver Cancer. 2016;16(2):69-81. Published online September 30, 2016
- DOI: https://doi.org/10.17998/jlc.16.2.69
- 1,015 Views
- 10 Downloads
- 1 Citation
-
Abstract
PDF
- Hepatocellular carcinoma (HCC) patients with portal vein tumor thrombosis (PVTT) have a extremely poor prognosis. According to the Barcelona Clinic Liver Cancer guideline, sorafenib is a standard therapy in this situation, but many clinicians still select locoregional therapy (LRT) such as transarterial therapy, external beam radiation therapy (EBRT), even surgical resection (SR) or combination of LRTs because the survival improvement by sorafenib is unsatisfactory. Based on recent meta-analysis and prospective study, transarterial chemoembolization (TACE) and transarterial radioembolization seem to be effective and safe therapeutic option that have comparable outcome to sorafenib. Recently large nationwide studies demonstrated that SR can be a potentially curative treatment in selected patients. Hepatic arterial infusion chemotherapy (HAIC) can be also good option, especially in Child class B patients based on small volume prospective studies. Moreover, multidisciplinary strategies based on the combination of LRTs (SR plus TACE, TACE + EBRT, TACE + Sorafenib, HAIC + EBRT etc.) may improve survival of HCC patients with PVTT. Finally we discuss individualized and tailored treatment strategies for different clinical situations.
-
Citations
Citations to this article as recorded by- Progress in Non-Surgical Treatment of Primary Hepatocellular Carcinoma with Combined Portal Vein Carcinoma Thrombosis
文豪 寇
Advances in Clinical Medicine.2023; 13(07): 11779. CrossRef
- Progress in Non-Surgical Treatment of Primary Hepatocellular Carcinoma with Combined Portal Vein Carcinoma Thrombosis
Case Reports
- A Case of Successful Hepatic Resection after Insufficient Response to Transarterial Chemoembolization and Radiation Therapy in Hepatocellular Carcinoma with Portal Vein Invasion
- Seong Kyun Na, Hyung Joon Yim, Sang Jun Suh, Young Kul Jung
- J Liver Cancer. 2016;16(2):118-122. Published online September 30, 2016
- DOI: https://doi.org/10.17998/jlc.16.2.118
- 939 Views
- 5 Downloads
-
Abstract
PDF
- Hepatocellular carcinoma (HCC) with portal vein invasion has a poor prognosis. Treatments such as transarterial chemoembolization (TACE), radiation therapy (RT), sorafenib are done as a first line treatment. But in case of incomplete response to first line treatment, there’s no established guideline about salvage treatment. We present a 47 year-old male who was diagnosed as HCC with portal vein invasion. He was treated with RT and repeated TACE, but remnant viable tumor was observed. Surgical resection was performed as a salvage treatment, and HCC was completely removed. He has been followed up over 3 years, but there was no recurrence.
- 3 Cases of Portal Vein Thrombosis in Hepatocellular Carcinoma and Liver Cirrhosis Treated with Anticoagulation
- Byung Moo Ahn, Eaum Seok Lee, Seok Hyun Kim, Byung Seok Lee, Heon Young Lee
- J Liver Cancer. 2015;15(1):57-63. Published online March 31, 2015
- DOI: https://doi.org/10.17998/jlc.15.1.57
- 1,318 Views
- 20 Downloads
- 1 Citation
-
Abstract
PDF
- The reported prevalence of PVT is in the range of 0.6-15.8% in patient with liver cirrhosis or portal hypertension. If the patient has hepatocellular carcinoma, thrombus is likely to be malignant thrombus. Malignancy, frequently of hepatic origin, is responsible for 21-24% of over all cases. The overall mortality rate of chronic PVT has been reported to be less than 10%, but is increased to 26% when associated with hepatocellular carcinoma and cirrhosis. However, no treatment guideline has been established on anticoagulant therapy for PVT in patients with concomitant hepatocellular carcinoma and cirrhosis. Because actually it is not easy to distinguish between malignant thrombus and benign thrombus in clinical aspect, PVT in hepatocellular carcinoma are still debatable whether or not treatment when it diagnosed. We present 3 cases of portal vein thrombosis successfully treated with anticoagulation in hepatocellular carcinoma and liver cirrhosis, and we include a literature review.
-
Citations
Citations to this article as recorded by- Evaluation of Low-Molecular-Weight Heparin for Treatment of Portal Vein Thrombosis in Liver Cirrhosis Patients
Ji Min Han, Youngil Koh, Sung Hwan Kim, Sung Yun Suh, Yoon Sook Cho, Jeong-Hoon Lee, Su Jong Yu, Jung-Hwan Yoon, Hye Sun Gwak
Medicina.2023; 59(2): 292. CrossRef
- Evaluation of Low-Molecular-Weight Heparin for Treatment of Portal Vein Thrombosis in Liver Cirrhosis Patients
- A Case of Achieving Partial Remission with Combination of Radiation Therapy and Sorafenib inChild-Pugh Class B Patients with Hepatocellular Carcinoma with Main Portal Vein Invasion and Lymph Node Metastasis
- Sang Youn Hwang, Seon-Mi Lee, Jung Woo Im, Joon Suk Kim, Sang Bu Ahn, Eun Kyeong Ji, Hyun-Cheol Kang, Cheol-Won Choi, Gwang-Mo Yang
- J Liver Cancer. 2014;14(2):120-126. Published online September 30, 2014
- DOI: https://doi.org/10.17998/jlc.14.2.120
- 969 Views
- 3 Downloads
-
Abstract
PDF
- Reserved liver function is one of the most important determinants of survivial in advanced hepatocellular carcinoma (HCC). Especially in cirrhotic patient with decompensated liver function, sorafenib for HCC with main portal vein invasion have limited efficacy and survival benefit. Therefore many clinicians or centers still try locoregional therapy (LRT) such as transarterial chemoembolization (TACE), radiation therapy (RT), or combination with LRT and sorafenib in this situation. However this multidisciplinary approach may increase treatment related toxicity such as liver failure, etc. Recently, studies for combination of RT and sorafenib for HCC with portal vein invasion have been tried and reported not only better therapeutic efficacy, but also more hepatic toxicity.Based on above suggestions, we herein offer our experience of a patient that although achieved survival gain via partial remission of intrahepatic tumor and main portal vein thrombosis and metastatic lymph node by combination therapy of RT and sorafenib, finally expired due to hepatictoxicity. Further study, maybe regarding a combination of locoregional and systemic therapy, is necessary on how to manage decompenstated cirrhotic patients with HCC with main portal vein invasion. (J Liver Cancer 2014;14:120-126)
- A Case of Perforation of Gastric Ulcer after Complete Remission of Huge Hepatocellular Carcinoma Invading Main Portal Vein with Combination Therapy of Stereotactic Body Radiation Therapy and Sorafenib
- Sang Youn Hwang, Seon-Mi Lee, Jung Woo Im, Joon Suk Kim, Sang Bu Ahn, Eun Kyeong Ji, Chul Won Choi, Gwang-Mo Yang
- Journal of the Korean Liver Cancer Study Group. 2014;14(1):46-52. Published online March 31, 2014
- DOI: https://doi.org/10.17998/jlc.14.1.46
- 1,259 Views
- 9 Downloads
- 1 Citation
-
Abstract
PDF
- Hepatocellular carcinoma (HCC) patients with main portal vein invasion have a poor prognosis associated with a median survival time of 2.7 months. Though many guidelines recommended sorafenib in HCC patients with macrovascular invasion (MVI), many clinicians or centers still select locoregional therapy (LRT) such as transarterial chemoembolization (TACE), radiation therapy (RT), or combination with LRT and sorafenib because the survival improvement by sorafenib only is expected to be shorter than that without MVI. However this multidisciplinary approach may increase treatment related toxicity such as liver failure etc. Stereotactic body radiation therapy (SBRT) is new technology providing very highly conformal ablative radiation dose for a small numbers (3-5 fractions) of large fraction size and is expected to new effective modality for HCC with MVI. Based on above suggestions, we herein offer our experience of a patient with perforation of radiation induced gastric ulcer after complete remission of tumor and main portal vein thrombosis by combination therapy of SBRT and sorafenib. Further study, maybe regarding a combination of locoregional and systemic therapy, is necessary on how to manage HCC patients with main portal vein invasion.
-
Citations
Citations to this article as recorded by- Novel management of expected post-radiotherapy complications in hepatocellular carcinoma patients: a case report
Sung Hoon Chang, Tae Suk Kim, Yong Hwan Jeon, Nuri Hyun Jung, Dae Hee Choi
Journal of Liver Cancer.2022; 22(2): 183. CrossRef
- Novel management of expected post-radiotherapy complications in hepatocellular carcinoma patients: a case report
- Living Donor Liver Transplantation for Hepatocellular Carcinoma with Portal Vein Tumor Thrombus
- YoungRok Choi, Kwang-Woong Lee, Hae Won Lee, Nam-Joon Yi, Kyung-Suk Suh
- Journal of the Korean Liver Cancer Study Group. 2013;13(1):62-64. Published online February 28, 2013
- DOI: https://doi.org/10.17998/jlc.13.1.62
- 1,220 Views
- 5 Downloads
-
Abstract
PDF
- Malignant portal vein thrombosis is a contraindication to liver transplantation for hepatocellular carcinoma because of the high risk of its recurrence and the poor patient survival. With a newly developed immunosuppressant and a chemotherapeutic agent, however, living donor liver transplantation can be considered for a patient of hepatocellular carcinoma, showing a slow growth rate and good response for transarterial chemoembolization. We report a HBV related liver cirrhosis patient with HCC and portal vein tumor thrombus who underwent living donor liver transplantation and survived without recurrence of hepatocellular carcinoma for 18 months in our center.
- A Case of Hepatocellular Carcinoma with Portal Vein Tumor Thrombi which was Performed Hepatectomy after Down-staging by Proton Therapy
- Hee-Jung Wang, Bong-Wan Kim, Wei-Kwang Xu
- Journal of the Korean Liver Cancer Study Group. 2011;11(1):56-59. Published online February 28, 2011
- 604 Views
- 1 Download
-
Abstract
PDF
- A case of hepatocellular carcinoma (HCC) with portal vein tumor thrombi (PVTT) which was performed hepatectomy after down-staging by proton therapy is reviewed. Generally, the recommended therapeutic strategy for this kind of HCC is radiation therapy, systemic or infusion anticancer chemotherapy. However, the response of HCC and its PVTT of this 56 year-old male patient was relatively good after 22 times of proton therapy, and we performed right hemihepatectomy on the concept of clinical trial under the informed consent of patient and his families. He is still alive without recurrence 15 months after hepatectomy. We suggest that hemihepatectomy with removal of PVTT could be an alternative strategy in the PVTT accompanied HCC cases who show good responses after the above generally recommended therapies.
- A Case of Hepatocellular Carcinoma Exhibited over Partial Response after Hepatic Arterial Infusion Chemotherapy
- Chang Wook Park, Young Lan Kown, Yong Jin Kim, Yoon Jung Kim, Hye Jin Seo, Kyung In Lee, Eun Soo Kim, Byung Kook Jang, Woo Jin Jeong, Kyung Sik Park, Kwang Bum Jo, Jae Seok Hwang, Young Hwan Kim, Jung Hyuk Kwon
- Journal of the Korean Liver Cancer Study Group. 2010;10(1):40-43. Published online June 30, 2010
- 589 Views
- 0 Download
-
Abstract
PDF
- Hepatocellular carcinoma (HCC) is one of the cancers with poor prognosis. Especially potal vein invasion is a grave prognostic indicator in the setting of HCC. There is currently no effective method for treatment of HCC with portal vein invasion. A 61-year-old female patient was diagnosed a massive HCCs in both hepatic lobe with portal vein thrombosis, based on computed tomography (CT) and increased tumor marker, α-fetoprotein. She was treated with intrahepatic arterial CDDP (10 mg on 1~5 day), 5-FU (250mg on 1~5 day) and leukovorin (12mg on 1~5 day) infusion via percutaneously implantable port system (PIPS) every 3 weeks, totally seven times. The patient was still living 6 months after first hepatic arterial infusion chemotherapy (HAIC) and follow-up CT showed partial response with necrosis of HCCs. We report here a case of advanced HCC with portal vein thrombosis that was effectively treated with HAIC via PIPS.
 First
First Prev
Prev


 Follow JLC on Twitter
Follow JLC on Twitter